Freudian Legacies
Sigmund Freud made significant contributions to our understanding of how the human mind works (Gay, 1988). Recently, however, his ideas have come under intense criticism. Eysenck (1985), MacMillan (1991), Fisher and Greenberg (1995), Webster (1995), Andrews and Brewin (2000) and Gomez (2005) review the issues (with different degrees of politeness and different conclusions). This post comments on some of Freud’s contributions.
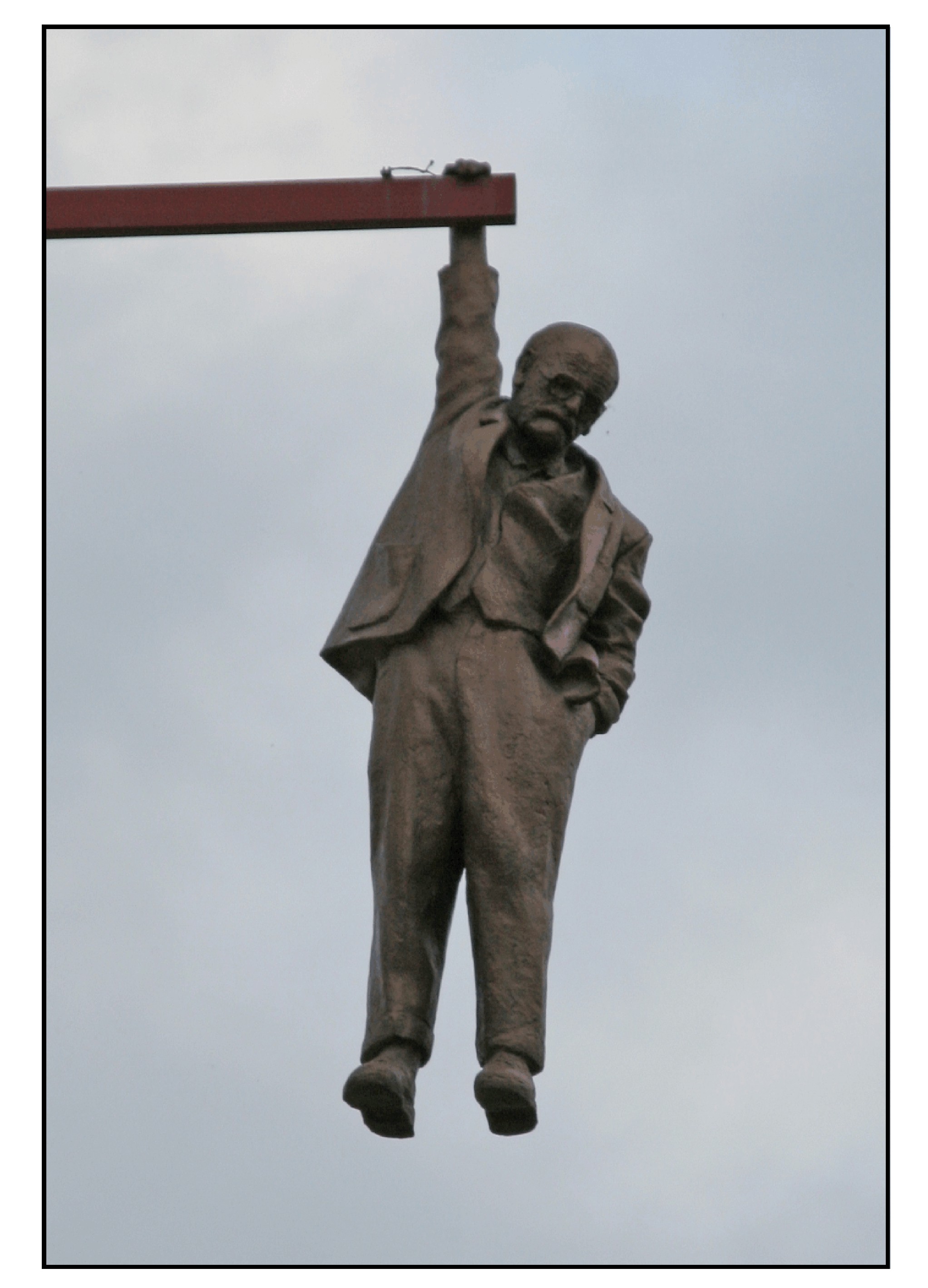
The photograph shows the Czech sculptor David Černý’s Hanging Man (1997) in its original location high above Husova Street in Prague. Copies have since been exhibited in various other cities. It is a life-size sculpture of Sigmund Freud, hanging from his right hand which grasps a beam projecting over the street. He seems unconcerned by his precarious position, his left hand remaining insouciantly in his pocket. Like most artists, Černý is noncommittal about the meaning of his art. According to some, the sculpture may represent the role of the intellectual in modern society. Freud goes often unattended, but when noticed he tends to shock. He considers ideas that are not grounded in the normal world; yet he is comfortable in his own thinking.
(i) The Unconscious
Freud proposed that the unconscious controls much of what we do. He did not invent the unconscious but he certainly demonstrated how great a role it plays in our thinking. Current scientific psychology has recognized how much of our thinking is unconscious. Most of our mental processes occur automatically without ever entering consciousness. Most of our memories are implicit and affect our thought and behavior without our ever noticing. Most of our motivations exercise their effects without our knowing. Westen (1999) reviews the extensive role of the unconscious in modern cognitive psychology.
The unconscious mediates what Freud called the “psychopathology of everyday life.” Unconscious activity often shows up in everyday speech, especially when we are not closely monitoring what we say. We currently use the term “Freudian slip” for those speech mistakes (parapraxes) with a sexual meaning: “we must encourage the breast (instead of best) and the brightest.” However, sex is not the cause of every mistake. There are often other things on our unconscious minds.
Free association, a key procedure in psychoanalytic therapy, may be a productive way for discovering what is active in the unconscious but not readily accessible. Relaxing on a couch and talking about the first thing that comes to mind may be as good a way as any for a patient and therapist to begin to talk.
The defense mechanisms described by Freud and his daughter Anna are the cognitive processes we use for handling stress. Repression, regression, sublimation, rationalization, and somatization all seem to be ways that the mind uses to cope with unwanted desires, to shield us from traumatic memories, and to reduce anxiety.
Dream recall may be an efficient way to trigger free associations. The experience of the dream may reflect what is active in our unconscious. Furthermore the retelling of a dream probably taps into all sorts of other mental information in addition to the actual dream. However, the interpretation of dreams is not the royal road to the unconscious. Freud proposed that a dream could represent the fulfillment of a repressed wish or it could mean exactly the opposite. In either case it could be disguised as something else. With such guidelines, dreams can be interpreted in an infinite number of ways.
Many of Freud’s dream-interpretations seem without any justification. Perhaps, the most famous of the dreams is Sergei Pankejeff’s recurrent nightmare of the white wolves in the tree outside his bedroom window (Gardiner, 1971). The patient drew a sketch of the dream for Freud during his 1910-1914 analysis. Many years later in 1964 he made a painting (shown below), which now hangs in the Freud Museum in Hampstead, London. Freud linked the dream to an eighteen-month-old infant’s memory of seeing his parents copulating. The interpretation seems far-fetched. Perhaps it betrays more the mental associations of the analyst than the repressed memories of the patient. The Wolfman later stated that the supposed memory was unlikely since his cot was in the nurse’s room and not his parent’s bedroom (Obholzer & Pankejeff, 1982, p. 36). We cannot consciously remember events before the age of about two or three years – “infantile amnesia.” Freud claimed that this specific memory from infancy was unconscious, but this was speculation without any corroboration.

(ii) Mechanisms of Memory
Freud’s views of childhood sexual abuse provide an intriguing case history on the difficulty of determining truth and the problems of memory (Gleaves & Hernandez, 1999). In his initial writings, Freud acknowledged that children had been sexually abused by their fathers, and suggested that this might be the cause of conversion hysteria. This formed the basis of the seduction theory. Later papers proposed that the abuse was fantasized rather than real, and that the fantasies were the effects of repressed desires on the part of the child. Freud has been both praised for recognizing the reality of childhood sexual abuse and criticized for later suppressing these ideas.
Why did Freud change his ideas? Was the change based on new evidence? Recent psychological investigations of false memories have shown how what we remember may not be what actually happened. Freud himself recognized that the physician may suggest the memories and that the patient may invent them. The actual events behind his patients’ histories are now impossible to determine. Freud’s change of theory may also have been caused by his (consciously or unconsciously) succumbing to social pressures. Viennese society was extremely strait-laced and did not wish to deal with the problem of childhood sexual abuse. One thing that is lost in the controversies is whether the new theory of repressed fantasies rather than repressed memories could explain the available data better than the old. Freud clearly thought that in many cases it did.
The incidence of childhood sexual abuse is likely higher than our sense of morality and decency would suggest. This has led to the idea that many psychological disorders in adulthood may be due to repressed memories of actual (not fantasized) abuse during childhood. Though such cases can occur, memories that are recovered during therapy are often not repressed memories of actual events but imagined memories suggested by the therapist (Crew, 1995).
If we accept that memories can be true or false, it is impossible to evaluate patient’s histories without some corroboration. Freud thought that the new theory was true because it led to success in treatment. Psychoanalytic success typically involved the cessation of symptoms once the patient and analyst came to a convincing interpretation of the symptoms in terms of repressed desires, and a re-integration of the personality so that such desires can be more effectively handled.
(iii) Psychoanalytic Therapy
Nowadays, the success of psychoanalytic treatment is not really clear. Psychoanalysis is resistant to scientific evaluation. In the last lecture of A General Introduction to Psychoanalysis Freud stated that each patient is unique, and “statistics would be valueless if the units collated were not alike.” People are too different from each other to allow comparable treatment groups. Family interactions are too complex to control. Anecdotal evidence of psychoanalytic cures abound. Yet analysts have a biased view of their ability, and patients do not wish to admit that the treatment has been unhelpful despite the huge investment of time and money. Objective outcome measurements are difficult to establish. We can measure improvement in the level of the symptoms and the quality of life. However, does improvement mean that a patient has recovered? Can a patient who has regained some semblance of normality still remain abnormally susceptible to stress?
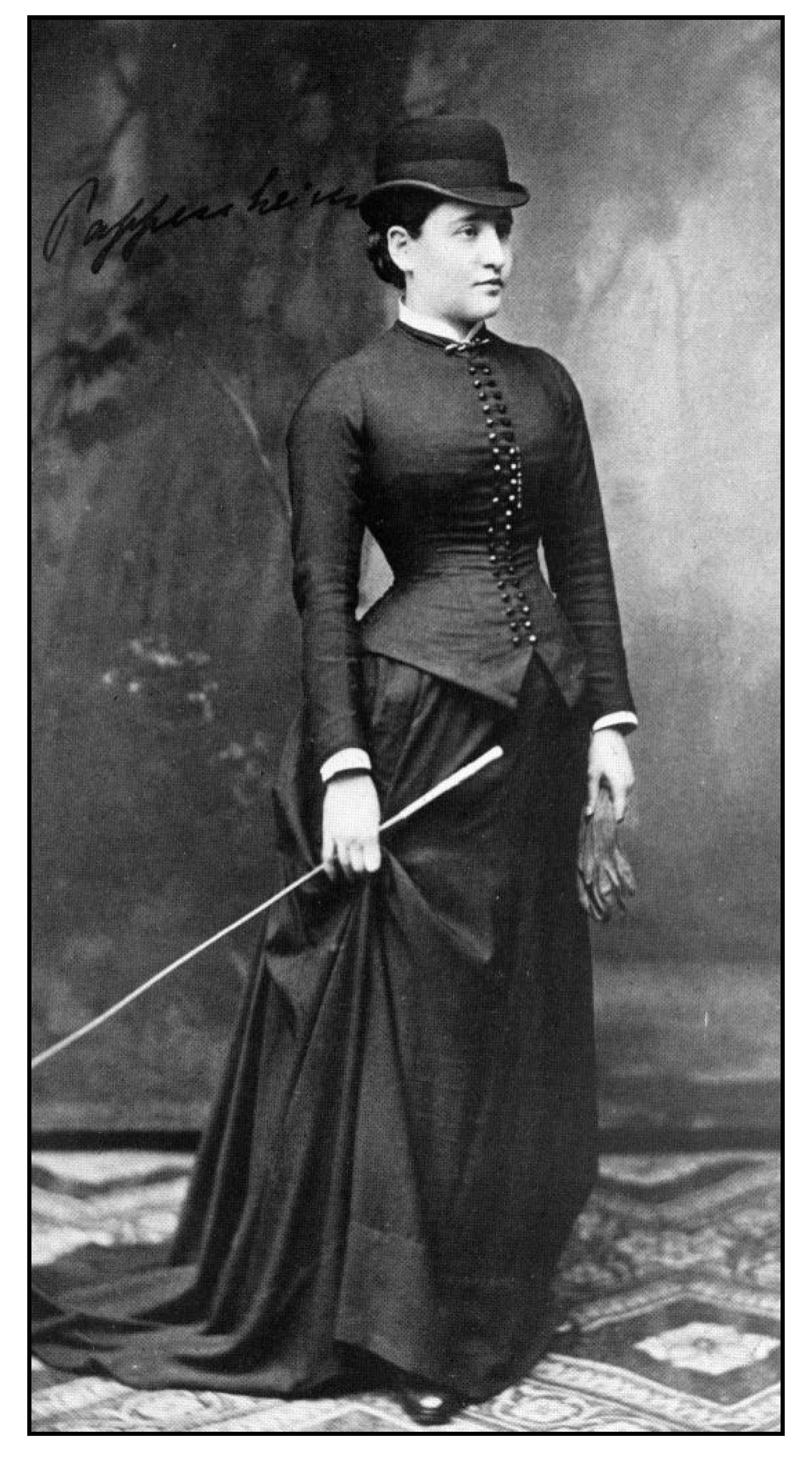
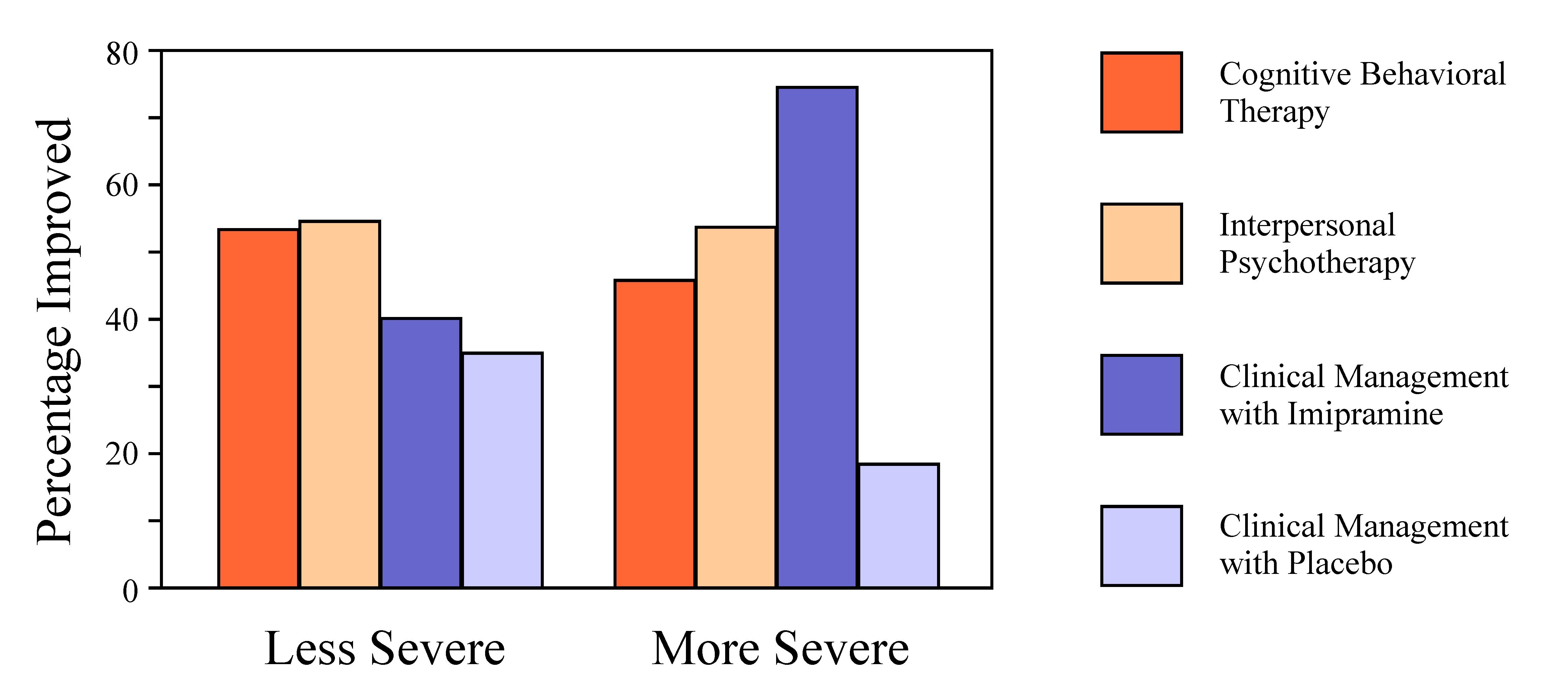
Studies evaluating psychotherapy using various outcome measurements have shown that it has a beneficial effect compared to no therapy (Wampold, 2001, 2007). The “talking cure” that began with Josef Breuer and Bertha Pappenheim works. However, the different types of therapy (those involving psychoanalytic theory and those not) are similar in the amount of benefit they provide. In patients with major depression, a large NIMH study (Elkin et al., 1989) compared two different psychotherapies (cognitive behavioral therapy and interpersonal psychotherapy), routine clinical management with imipramine and routine clinical management with placebo. The psychotherapy sessions were conducted weekly and lasted one-hour. The clinical management sessions were also weekly and lasted 20-30 minutes. The diagram shows some of the results, based on one of the several scales used in the study. All “treatments” led to improvement, even the placebo. The two psychotherapies and the active pharmacological treatment tended to be significantly better than placebo (though the tests were borderline and varied with the scales used to rate the severity of the depression). Part of the placebo effect may have been related to the passage of time, and part to the minimal psychotherapy involved in the once weekly brief meetings with the physician. The pharmacological treatment condition was better in patients with more severe depression. The results were variable and the differences between conditions were statistically borderline (and varied with the scales).
The study is typical. Psychotherapy has a beneficial effect. However, this effect is variable and sometimes different to demonstrate. Furthermore, there are often no clearly demonstrable differences between different types of therapy.
 Bruce Wampold (2001) described the lack of statistical difference between different therapies as the “Dodo bird verdict,” quoting an earlier paper of Saul Rosenzweig (1936). The reference is to Chapter 3 of Lewis Carroll’s Alice in Wonderland. When asked to determine who had won the “caucus-race” (a competition with no rules or measurements), the Dodo bird thought for a long while and finally decided that “Everybody has won, and all must have prizes”
Bruce Wampold (2001) described the lack of statistical difference between different therapies as the “Dodo bird verdict,” quoting an earlier paper of Saul Rosenzweig (1936). The reference is to Chapter 3 of Lewis Carroll’s Alice in Wonderland. When asked to determine who had won the “caucus-race” (a competition with no rules or measurements), the Dodo bird thought for a long while and finally decided that “Everybody has won, and all must have prizes”
The general idea of the talking cure is good, but it seems much less used in psychiatry in recent years, particularly in North America. This is unfortunate since for non-psychotic mental disorders the talking cure is probably as good as any pharmacological treatment. Even for psychosis, where medication is essential, the talking cure still helps. Nowadays, the interactions between psychiatrist and patient often serve only to assess symptoms, adjust medications and monitor side-effects. Psychotherapy (of whatever kind) is often not the primary activity.
The fact that all therapies work regardless of the type suggests that the beneficial effect is due to the interaction between the patient and a therapist. What makes a therapist good and the therapy beneficial remains difficult to determine. Clearly the therapist should be rational, sympathetic and supportive. The precise system of therapy does not seem to matter. Perhaps there may be some interaction with the personality of the patient. Some patients may do better with some system of therapy than with another. The therapist must have some bona fide training. The patient should not be treated by any mad charlatan who claims to be a therapist. And we need further evidence-based studies will determine which therapy is better for which patient (Hunsley & DiGiulio, 2002).
Most of the studies comparing different kinds of psychotherapy consider periods of time much briefer than used in classical psychoanalysis. “Psychodynamic therapy” is informed by psychoanalytic ideas but much briefer and much less intense. Although earlier studies have found otherwise, a recent meta-analysis has suggested that a prolonged course of analysis lasting for a year or more has no more benefit than a brief period of therapy lasting several weeks (Smite al al., 2012). On any cost-benefit evaluation, however, classical psychoanalysis involving multiple meetings per week and lasting over multiple years would fare very poorly.
The French Institute of Health recently evaluated published scientific studies of three different types of psychotherapy: psychodynamic therapy, cognitive behavioral therapy and family counseling. Their report (INSERM, 2004) proposed that cognitive behavioral therapy was the best approach to many different mental disorders and that psychodynamic therapy was never the preferred treatment. The report triggered a tremendous controversy (Meyer, 2005; Miller, 2006). Psychoanalysts claimed that a treatment that involved reprogramming and conditioning was inhumane; the opposition said that psychoanalysis was pseudoscience. Cognitive behavioral therapy (Beck, 2011) is designed to help patients cope with their symptoms and prevent their exacerbation. Symptoms are alleviated by training the patients to re-interpret the situations under which these symptoms become manifest. This type of therapy is clearly going to do well on studies with outcome measures that assess the severity of symptoms. The goal of psychoanalysis is a long-term re-education or re-integration of the personality. Psychoanalytic therapy might have done better with outcome measures that assess a patient’s understanding of self and of others (e.g. Berggraf et al., 2014)
(iv) Addiction to therapy
One of the difficulties with any psychotherapy is that it fosters an emotional dependence on the therapist that can become unhealthy. The patient may become unable to live without a weekly session with the therapist. This problem was recognized early in the history of psychoanalysis. The Viennese satirist Karl Kraus (1913) proposed that psychoanalysis is the mental illness whose cure it purports to be (“Psychoanalyse ist jene Geistekrankheit, für deren Therapie sie sich hält”). Even with client-centered therapy, the therapist generally remains the dominant person in the interaction. Psychotherapy has some relations to religion, with confession followed by interpretation rather than absolution.
Some therapies become cults. The patient becomes enslaved to a particular system of thought. Scientology started as a treatment procedure, and therapy continues as a main activity in the movement. Scientology proposes that a person’s achievements may be held back by memories or “engrams” (from early childhood or from another life). The goal of the therapy is to discover (or “audit”) these impediments by using an “e-meter” (a simple psychogalvanometer). Once identified these impediments can be removed (or “cleared”) by therapy, allowing the patient to become a more complete human being (or “thetan”). Therapies are paid for – a patient who is not willing to pay is not going to be cured. As far as I can understand, scientology is nonsense. It exists not to cure the sick but to allow an elite to make money and to exert power.
Although clearly different, scientology and psychoanalysis have some similarities. Both have a background theory that has not been experimentally tested. Both focus on the handling of anxiety. Both are based on a charismatic leader. Psychoanalysis can be beneficial and Scientology is malignant, but the similarities are very worrisome.
(v) Overview
What then is psychoanalysis? It is a system of thought and a way of treatment based on an imaginative interpretation of human development and culture. Psychoanalytic treatment interprets what has happened to a patient to lead to the present situation, and attempts to re-integrate the patient’s personality to reduce the conflict between unconscious desires and ideal goals. Even though Freud considered his work as science, it makes no hypotheses that can be refuted. In a sense anything can be explained. A dream may sometimes represent a wish fulfillment; at other times defense mechanisms may have sufficiently distorted its content to represent the complete opposite of wish-fulfillment.
Psychoanalysis has made significant contributions to our culture. First is the freeing of our minds so that we can recognize our desires, especially those that are sexual in nature. Second is the recognition that most of what we think and do is the result of unconscious processing. Third is the idea that talking to a sympathetic therapist can help us to understand ourselves and to attenuate the stress that results when desires and ideals come into conflict. Fourth is the description of a life narrative wherein we can realistically cope with our unconscious desires.
Psychoanalysis is imaginative rather than scientific According to John Irving, “Sigmund Freud was a novelist with a scientific background” (Plimpton, 1988). Freud’s interpretation of human development according to the story of Oedipus is a powerful metaphor. The meaning is in the way it helps us to see our life, not in how it represents what actually happens. The story of Oedipus encapsulates many aspects of the human condition. (The illustration shows Oedipus being questioned by the Sphinx on a drinking cup from around 470 BCE, Vatican museums, photographed by Carole Raddato).

Jacques Lacan said many outrageous things about psychoanalysis. Within his hyperbole there are germs of truth. The post concludes with two quotations from his seminars:
La psychanalyse est à prendre au sérieux, bien que ce ne soit pas un science … parce que c’est irréfutable … c’est un pratique du bavardage. (Lacan 1979) [Psychoanalysis is to be taken seriously even though it is not a science … because its propositions cannot be falsified … it is an exercise in conversation. (I have attenuated the translation of “bavardage,” which means “chattering” or “gossip” to better portray the idea of the “talking cure” )]
Le psychanalyste ne doit jamais hésiter a délirer. (Lacan, 1977) [The psychoanalyst must never hesitate to imagine freely. (I have attenuated the hyperbolic “délirer” which means “become delirious”).
Psychoanalysis is an imaginative way of looking at human life that can help patients in distress and suggest ways to understand the workings of the mind.
Andrews, B., & Brewin, C. R. (2000). Freud in a modern light. (Special issue). The Psychologist, 13:605-623.
Beck, J. S. (2011). Cognitive behavior therapy: basics and beyond. New York: Guilford Press.
Berggraf, L., Ulvenes, P. G., Hoffart, A., McCullough, L., & Wampold, B.E. (2014): Growth in sense of self and sense of others predicts reduction in interpersonal problems in short-term dynamic but not in cognitive therapy. Psychotherapy Research, in press.
Crews, F. C. (1995). The memory wars: Freud’s legacy in dispute. New York: New York Review of Books.
Elkin, I., Shea, M.T., Watkins, J.T., Imber, S.D., Sotsky, S.M., Collins, J.F., Glass, D.R., Pilkonis, P.A., Leber,W.R., Docherty, J.P., Fiester, S.J., & Parloff, M.B. (1989). National Institute of. Mental Health treatment of depression collaborative research program: general effectiveness of treatments. Archives of General Psychiatry, 46, 971–982.
Eysenck, H. J. (1985). Decline and Fall of the Freudian Empire. New York: Penguin.
Fisher, S., & Greenberg, R.P. (1996). Freud scientifically reappraised: Testing the theories and the therapy. New York: Wiley
Freud, S. (1922, translated by Riviere, J., 1935). A general introduction to psychoanalysis. New York: Liveright.
Gardiner, M. (Ed.). (1971). The Wolf-Man by the Wolf-Man. New York: Basic Books (Contains Freud’s original case history from 1918 and an interview with the patient)
Gay, P. (1988). Freud: A life for our time. New York: Norton.
Gleaves, D. H, Hernandez E. (1999). Recent reformulations of Freud’s development and abandonment of his seduction theory: historical/scientific clarification or a continued assault on truth? History of Psychology, 2, 304-54.
Gomez, L. (2005). The Freud wars: An introduction to the philosophy of psychoanalysis. London: Routledge.
Hunsley, J., & Di Giulio, G. (2002). Dodo bird, phoenix, or urban legend? The question of psychotherapy equivalence. Scientific Review of Mental Health Practice, 1, 11-22.
INSERM Collective Expert Reports (2004). Psychotherapy: Three approaches evaluated. Paris: Institut national de la santé et de la recherche médicale.
Kraus, K. (1913) Die Fackel Nr 376/377, p. 21.
Lacan, J. (1977). Ornicar ? No 9, p. 17
Lacan, J. (1979). Ornicar ? No 19, p. 5
Macmillan, M. (1991). Freud Evaluated: The Completed Arc. Amsterdam: North Holland.
Meyer, C. (Ed.) (2005). Le livre noir de la psychanalyse, Paris: Les Arènes.
Miller, J.-A. (Ed.) (2006). L’anti-livre noir de la psychanalyse. Paris: Le Seuil.
Obholzer, K., & Pankejeff, S. (1982). The Wolf-Man: Conversations with Freud’s patient – sixty years later. New York: Continuum.
Plimpton, G. (1988) Interview with John Irving. In: Writers at Work: The Paris Review Interviews, Eighth Series. New York: Penguin.
Rosenzweig, S. (1936). Some implicit common factors in diverse methods of psychotherapy. American Journal of Orthopsychiatry, 6, 412–415.
Smit, Y., Huibers,M. J., Ioannidis, J. P., van Dyck, R., van Tilburg, W., & Arntz, A. (2012) The effectiveness of long-term psychoanalytic psychotherapy – a meta-analysis of randomized controlled trials. Clinical Psychology Review, 32, 81-92
Wampold, B. E. (2001). The great psychotherapy debate: Models, methods, and findings. Mahwah, NJ: Lawrence Erlbaum Associates.
Wampold, B. E. (2007). Psychotherapy: the humanistic (and effective) treatment. American Psychologist, 62, 855-873.
Webster, R. (1995). Why Freud was wrong: Sin, science, and psychoanalysis. New York, NY: BasicBooks.
Westen, D. (1999). The scientific status of unconscious processes: is Freud really dead? Journal of the American Psychoanalytic Association, 47, 1061-1106.